Applications of Artificial Intelligence in Systemic Lupus Erythematosus: Addressing Disease Heterogeneity to Personalize Care

Autoimmunity is a condition that develops when the immune system, which normally protects us against invading pathogens such as bacteria and viruses, mistakenly attacks our own healthy tissues [1]. Normally, our immune system is kept from turning against us by a mechanism known as tolerance, but when this process is disturbed, it can no longer distinguish self from non-self and begins attacking healthy tissues. Understanding the cellular and molecular details of immune tolerance has been an area of intense research. In recognition of the foundational importance of this field, the 2025 Nobel prize in physiology and medicine was awarded to Dr. Mary E. Brunkow, Dr. Fred Ramsdell and Dr. Shimon Sakaguchi, three scientists who discovered T regulatory (Treg) cells, which play a key role in one aspect of immune tolerance.
Autoimmune diseases can also be thought of in terms of which part of the immune system is doing the attacking. In B cell-dominated diseases, autoantibodies that bind self-tissues are important contributors to the development of clinical abnormalities. In contrast, some diseases are T cell-dominated, driven mainly by autoreactive T lymphocytes. For instance, type 1 diabetes and rheumatoid arthritis have long been viewed as T cell diseases. There are even conditions where innate immune cells (like neutrophils or monocytes) are the main culprits. For example, several “autoinflammatory” diseases like familial Mediterranean fever involve overactive innate immune cells. The participation of distinct cell types in autoimmunity has led to the development of cell type-directed therapies.
Systemic lupus erythematosus (SLE) is a classic systemic autoimmune disease that originates as a result of perturbation in immune tolerance [2]. SLE can be considered to be a B cell-dominated disease, where high levels of antibodies against self-antigens cause widespread inflammation. In SLE, patients produce high titers of autoantibodies, especially against components of the cell nucleus. These autoantibodies form immune complexes that cause damage to multiple organ systems by activating complement and inciting inflammation. SLE affects the skin, joints, kidneys, blood, brain and other tissues. Its course and severity are highly variable; for example, some patients only have mild skin and joint symptoms, while others develop life-threatening organ damage. SLE overwhelmingly affects women of child-bearing age, illustrating the complex interplay of genetics, hormones and the environment in autoimmunity.
SLE Therapeutics
Treating lupus involves a combination of approaches to dampen the overactive immune system and protect organs. Almost all patients start with hydroxychloroquine (an anti-malarial drug), since this is generally safe and effective for mild disease. During flares or more severe illness, doctors use corticosteroids (like prednisone) to rapidly control inflammation. Patients with serious organ involvement (e.g. kidney or brain) are given stronger immunosuppressant drugs such as azathioprine, methotrexate, mycophenolate mofetil or cyclophosphamide. In the last few years, new targeted therapies have been approved. Notably, two monoclonal antibodies are now FDA-approved for lupus: belimumab, which blocks the B cell activation factor (BAFF), and anifrolumab, which blocks the type I interferon (IFN) receptor. These biologics can reduce disease activity in many patients. For lupus that affects the kidneys (lupus nephritis), belimumab has been shown to improve kidney outcomes, and a new oral drug called voclosporin (a calcineurin inhibitor) was FDA-approved in 2021 to help protect kidney function [3].
Beyond these approved therapies, B cell-targeted monoclonal antibodies directed against cluster of differentiation 20 (CD20) have emerged as important treatment options, though they remain off-label for lupus. Rituximab, a chimeric anti-CD20 monoclonal antibody, is the most widely used in this class and has shown clinical benefits in refractory and severe lupus, particularly lupus nephritis, in numerous open-label studies and real-world clinical practice [4]. Despite failing to meet primary endpoints in two major randomized controlled trials (EXPLORER for non-renal SLE and LUNAR for lupus nephritis), rituximab has demonstrated significant efficacy in reducing disease activity, achieving renal remission rates, and serving as a steroid-sparing agent in many patients with treatment-resistant disease. Clinical experience shows that rituximab induces B cell depletion in approximately 95% of patients with a relatively good safety profile, and it is recommended by the American College of Rheumatology as a second-line treatment for refractory class III and IV lupus nephritis.
Newer generation anti-CD20 antibodies have also been investigated in lupus. Obinutuzumab, a glycoengineered type II humanized anti-CD20 antibody with enhanced B cell killing capacity, demonstrated superiority to placebo in achieving complete and overall renal responses in the phase II NOBILITY trial for proliferative lupus nephritis. This led to a global phase III REGENCY study, and the FDA accepted a supplemental Biologics License Application for obinutuzumab in lupus nephritis in March 2025, with a decision expected by October 2025. Ofatumumab, a fully human anti-CD20 antibody, has shown promise as a well-tolerated alternative for patients who are rituximab-intolerant, with successful B cell depletion and clinical responses reported in smaller cohorts with lupus nephritis and other severe manifestations. Other anti-CD20 antibodies such as ocrelizumab have also been evaluated, though with more limited data in lupus.
All together, these standard and novel treatments have greatly expanded our options. However, lupus remains unpredictable. It has been noted that lupus affects the immune system differently in different people, so a therapeutic intervention that works well for one person may not be very effective in another. This helps explain why even with multiple drugs available, not every patient achieves remission – a challenge we explore next in the discussion of lupus heterogeneity.
Addressing Heterogeneity in Lupus
One of the biggest challenges in treating lupus is its cellular and molecular heterogeneity. The fact that patients differ at these levels is reflected in the variations observed in clinical manifestations and disease outcomes. Think of it like this: while lupus patients may share some common clinical manifestations, the underlying mechanisms driving the disease pathology can be quite different in one patient compared to the next. They might involve different molecular pathways, distinct gene expression patterns, and different immune cell activity orchestrated by genetic and environmental determinants.
Researchers have realized that lupus patients can actually be grouped into distinct subtypes based on specific cellular and molecular characteristics. For example, a subtype with pathogenicity driven by monocyte and neutrophil activity, or a subtype marked by high type I IFN levels. This diversity helps explain why some patients respond well to certain treatments while others don't. To address this complexity, scientists are working on precision medicine approaches that use genetic and epigenetic markers, autoantibody profiles, cytokine levels and other biomarkers to better classify lupus patients. By identifying which cellular and molecular pathways are most active in each individual patient through techniques like single-cell RNA sequencing (scRNA-seq) and immune phenotyping, doctors may eventually be able to tailor treatments more precisely to match each person's unique disease signature, moving away from the one-size-fits-all approach that has historically made lupus difficult to treat effectively.
Decoding the Hidden Cellular and Molecular Signatures with Artificial Intelligence
Modern analytic methods (whole-genome sequencing, single-cell and bulk RNA expression, immune cell phenotyping, etc.) generate vast amounts of data that encapsulate hidden signatures of SLE pathogenesis and progression. Advanced artificial intelligence (AI) and machine learning tools are being used to deconvolute these signals to reveal important determinants of disease. Some of the approaches are summarized below:
- Transcriptomic Profiling and Machine Learning: Lupus has been subjected to transcriptome profiling using microarray technology or RNA-seq. These large pools of gene expression data from thousands of patients are analysed by integrative methods such as gene set variation analysis (GSVA) and machine learning models to identify enriched pathways that correlate with disease phenotype. The Lipsky group applied these methods to classify lupus patients into eight distinct molecular endotypes [5]. Each endotype showed enrichment of different pathways and involvement of different cell types and correlated with disease activity.
- Mapping functional diversity of T cells through gene-expression programs: Instead of clustering cells just by type, new pipelines (e.g. T-Cell AnnoTator or TCAT) disentangle T cell transcriptomes into gene-expression programs (GEPs) that represent functional states. A study from Harvard Medical School analysed ~1.7 million T cells across many lupus samples and identified 46 distinct T cell functional programs (such as proliferation, cytotoxicity, exhaustion, effector polarization, etc.) present in these samples, further substantiating the molecular heterogeneity described in the previous section [6]. These AI-driven methods can then automatically annotate individual cells and cluster cells with similar GEP activity to identify enrichment of cellular processes associated with the disease. For example, TCAT’s catalogue of T cell GEPs can accurately predict T cell subsets and activation states in new datasets, outperforming traditional clustering.
- Multi-omics integration: Combining transcriptomics with immunophenotyping (fluorescence or mass cytometry) adds another layer to the molecular phenotype of diseases. A recent study stratified 235 patients with various immune diseases (including SLE) into two clusters based on B cell immunophenotypes. They then overlaid transcriptomic data on these clusters. One cluster, enriched in mature or memory B cells, showed enrichment of BAFF signalling. The second cluster, enriched in naïve B cells, showed pathways related to B cell receptor (BCR) signalling [7]. Such integrated AI-driven analyses can uncover both quantitative and qualitative patterns that are often missed by conventional methods.
- Automated cell-state annotation: Tools like TCAT demonstrate that AI can annotate complex cellular states without manual gating. In practice, this means a computer program can take raw single-cell data and label which cells are, say, T helper 17 (Th17)-like or exhausted T cells, based on learned gene programs [6]. These automated annotations make the hidden heterogeneity of the immune response visible and quantifiable.
In summary, AI and machine learning are now able to sift through lupus datasets like bulk transcriptomes, scRNA-seq, cytometry, etc., and pull out the underlying immune signatures. These analyses reveal the “molecular fingerprint” of each patient’s disease, enabling objective classification and comparison.
From Mechanisms to Medicine – Therapeutic Implications of AI-Driven Insights
Decoding these signatures has direct clinical relevance as described in the examples below.
The multi-omics study on B cell immunophenotypes mentioned earlier highlights how molecular signatures can guide patients to personalized therapy. Cluster 2 in this study, characterized by high levels of naïve B cells, correlated with higher SLE activity and more frequent flares and worse prognosis. These patients are likely to benefit from B cell depletion therapies such as anti-CD20 antibody Rituxan or B cell-targeted chimeric antigen receptor (CAR)-T cell therapies, many of which are currently in clinical trials. Similarly, Cluster 1 patients enriched in mature B cells are likely to benefit from anti-BAFF therapies such as Belimumab, which blocks BAFF signaling in B cells [7].
T cell signatures add yet another layer of therapeutic insight. For example, aberrant activation and defective regulatory programs in T cells are important factors in lupus pathogenesis. Evidence from programmed cell death protein 1 (PD-1) knockout mice, the contraindication of checkpoint inhibitors in autoimmune settings, and the protective effects of programmed death-ligand 1 (PD-L1)–Fc fusion proteins all highlight that uncontrolled T cell activation exacerbates disease. In this context, identifying dominant T cell programs such as aberrant cytotoxic T cells, Th17 cells or exhaustion-associated states can reveal which pathogenic pathways are active in a given patient. Such insights may guide the development of T cell–specific mitigation strategies, including approaches that restore inhibitory signaling, enhance regulatory T cell stability, or re-establish immune tolerance.
Overall, immune profiling at a cellular and molecular level is paving the way towards precision therapy by decoding the disease heterogeneity and aligning drug mechanisms with patient-specific enriched immune pathways. As one research group noted, integrating immunophenotypes with transcriptomic data provides a more refined classification system that can meaningfully inform treatment planning. In lupus, this evolution signifies a shift from a “try steroids and see” approach to a rational, signature-based method of choosing therapies that best fit each individual’s disease features.
ThinkBio’s Approach to Developing a Personalized Care System
ThinkBio.Ai® envisions that the future of healthcare will be a mix of technology and biology that will transform how we understand and treat complex diseases like lupus. Today, physicians and researchers face a significant challenge when dealing with lupus and other autoimmune diseases: even when patients share a diagnosis, their symptoms, responses to treatment, and disease progression can differ greatly. ThinkBio.Ai® wants to tackle this challenge by using AI to make sense of these differences. Its team of experts in immunology, bioinformatics and advanced computational methods will mine public and proprietary repositories containing multiple types of data - genomics, transcriptomics, immunophenotyping, etc. - and use AI tools to reveal patterns that are too complex for the human mind to discern on its own. The results of such analyses will help researchers understand the hidden logic behind lupus variability.
ThinkBio’s strategy for implementing AI in lupus stratification has been outlined in Figure 1. Beyond lupus, the potential for discovering hidden molecular patterns will influence how we approach many other immune-related diseases.
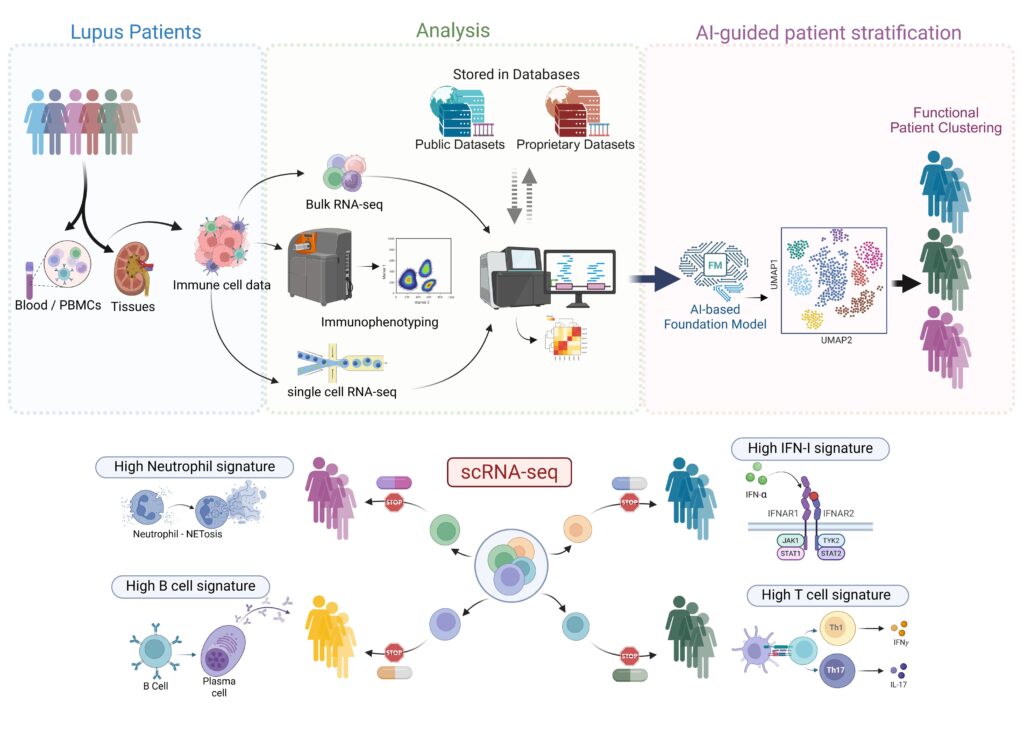
Figure 1: AI-assisted multi-omics approach for lupus patient stratification. Immune cell data obtained from lupus patient blood and tissue samples are analysed through bulk RNA-seq, scRNA-seq, and immunophenotyping. The resulting datasets, stored across public and proprietary repositories, can be accessed under appropriate data-sharing agreements and leveraged to train AI-based foundation models for functional patient clustering. The lower panel illustrates how single-cell transcriptomic profiling captures immune cell heterogeneity and delineates pathway-specific signatures, enabling mechanistic insights and facilitating precision disease management.
Conclusion – A New Era of Precision Autoimmunity Management
The convergence of AI and immunology is ushering in a new era in our understanding of autoimmunity. The capacity of AI to integrate and interpret vast, heterogeneous datasets represents a transformative step toward deciphering the complex biological interactions that drive disease onset and progression. By revealing previously hidden molecular patterns and immune network dynamics, AI is enabling a more precise characterization of patient subgroups and disease trajectories. ThinkBio, with its suite of proprietary AI tools, knowledge platforms, and integrative solutions, is well positioned to translate these insights into tangible advances in precision medicine for lupus and other autoimmune diseases.
References :
- Sakaguchi S, Mikami N, Wing JB, et al. Regulatory T cells and human disease. Annu Rev Immunol. 2020; 38:541-566. doi:10.1146/annurev-immunol-042718-041717
- Caielli S, Wan Z, Pascual V. Systemic lupus erythematosus pathogenesis: interferon and beyond. Annu Rev Immunol. 2023; 41:533-560. doi:10.1146/annurev-immunol-101921-042422
- Fanouriakis A, Kostopoulou M, Andersen J, et al. EULAR recommendations for the management of systemic lupus erythematosus: 2023 update. Ann Rheum Dis. 2024; 83:15-29. doi:10.1136/ard-2023-224762.
- Lee DSW, Rojas OL, Gommerman JL. B cell depletion therapies in autoimmune disease: advances and mechanistic insights. Nat Rev Drug Discov. 2021; 20:179-199. doi:10.1038/s41573-020-00092-2
- Hubbard EL, Bachali P, Kingsmore KM, et al. Analysis of transcriptomic features reveals molecular endotypes of SLE with clinical implications. Genome Med. 2023; 15:84. doi:10.1186/s13073-023-01237-9
- Kotliar D, Curtis M, Agnew R, et al. Reproducible single-cell annotation of programs underlying T cell subsets, activation states and functions. Nat Methods. 2025; 22:1964-1980. doi:10.1038/s41592-025-02793-1
- Izuka S, Komai T, Itamiya T, et al. Integration of transcriptome and immunophenotyping data highlights differences in the pathogenetic kinetics of B cells across immune-mediated disease. RMD Open. 2025;11: e005310. doi:10.1136/rmdopen-2024-005310